Hanyu Frontier
Structural Heart Disease
Frontier Explorer
NEW OPPORTUNITIES FOR INNOVATIVE INVESTMENT IN
STRUCTURAL HEART DISEASE
STRUCTURAL HEART DISEASE

Structural Heart Disease
Frontier Explorer
Recently, the cardiovascular surgery team led by Professor Chen Hao at Chongqing People’s Hospital successfully and independently completed a ValveClamp® transapical transcatheter edge-to-edge repair (TEER) for severe mitral regurgitation in an 81-year-old high-risk patient.
This achievement marks a significant milestone for the hospital in the field of minimally invasive and structural heart disease interventions.

Gender: Male
Age: 81 years
Chief Complaint: Dyspnea and fatigue after exertion for 1 year, worsening for 1 month
Preoperative Diagnosis: Heart failure (NYHA Class III); severe mitral regurgitation; cardiomegaly
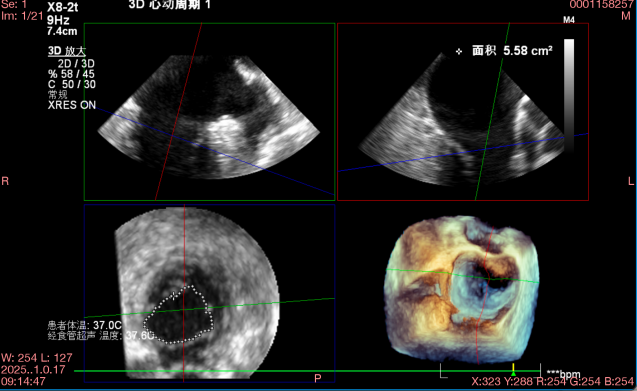
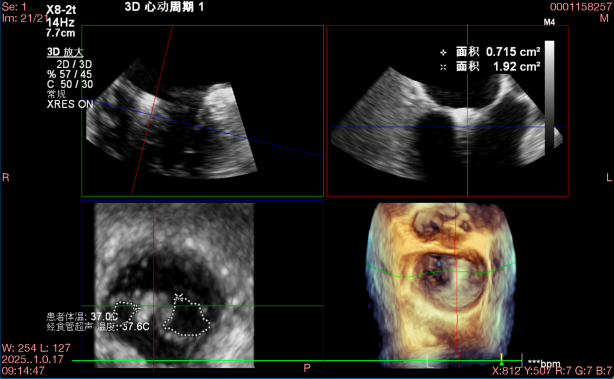
Degenerative mitral regurgitation (DMR) with A2–A3 prolapse and flail motion (prolapse height: 17 mm; flail gap: 7 mm) and P3 prolapse.
The regurgitation jet was mainly located in segments 2–3, with severe MR (4+) and a vena contracta of 6 × 17 mm.
Measurements: A3 18 mm, P3 9 mm, A2 24 mm, P2 14 mm, annular anteroposterior (AP) diameter 32 mm, mitral valve area (MVA) approximately 5.6 cm².
Marked left atrial and left ventricular enlargement was observed.
Under general anesthesia, the ValveClamp® device was successfully implanted via a transapical approach.
The multidisciplinary team worked in close coordination, with real-time transesophageal echocardiography guiding every step of the procedure.
A single Type IIIf clip was precisely deployed at the 2–3 segment, achieving an optimal grasp on the first attempt.
The grasping lengths were 12 mm (anterior leaflet) and 10 mm (posterior leaflet), reducing regurgitation from 4+ to 1+.
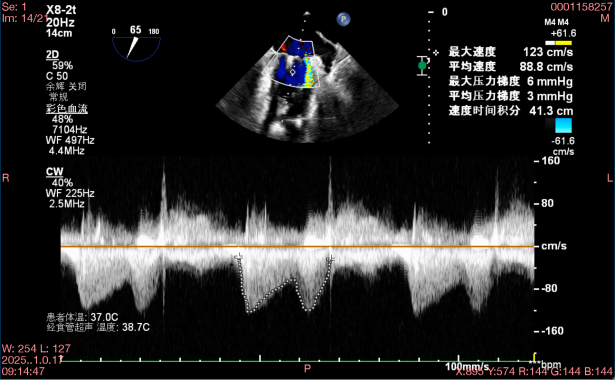
The total device manipulation time was 30 minutes, and the mean transmitral gradient post-procedure was 3 mmHg.
Preoperative Regurgitation 
Postoperative Regurgitation



TEL: 021-6219 9996
ADD:Building 14, Gemdale Weixin Technology Park, 1288 Zhongchun Road, Minhang District, Shanghai